Objectives: To evaluate the effects of MI combined with PNI on the quality of life, self-efficacy, psychological state, and sleep quality of patients with GERD. Methods: 60 GERD patients were enrolled based on inclusion and exclusion criteria and randomly assigned to the observation (30 cases) or control groups (30 cases). The observation group underwent MI combined with PNI, while control group received conventional nursing interventions. The changes in inflammatory response-related indicators were compared between two groups. The reflux disease questionnaire (RDQ), symptom self-rating scale (SCL-90), self-efficacy scale (GSES), simple SF-36 scale and Pittsburgh sleep quality index scale (PSQI) were employed to assess the patient's conditions before, three months following and after nursing. Results: Baseline inflammatory markers and scale scores showed no significant between-group differences. After 3 months, the observation group demonstrated significant reductions in these inflammatory markers compared with baseline and the control group. At the same time point, SCL-90 scores decreased across multiple domains, GSES scores improved, and SF-36 scores increased in several dimensions. PSQI scores were also significantly lower in the observation group, indicating better sleep quality. Conclusion: MI combined with PNI may reduce inflammation, relieve negative emotions, and enhance self-efficacy, quality of life, and sleep in GERD patients.
| Published in | Clinical Medicine Research (Volume 15, Issue 1) |
| DOI | 10.11648/j.cmr.20261501.12 |
| Page(s) | 6-18 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Gastroesophageal Reflux Disease, Emotions, Motivational Interviewing, Nursing Care
Baseline information | Control group (n=30) | Observer group (n=30) | Statistic | p |
|---|---|---|---|---|
Age (year) | 43.20±6.52 | 43.70±6.48 | -0.298 | 0.767 |
Gender | ||||
Males | 13(43.33) | 15(50.00) | <i></i>2=0.268 | 0.605 |
Female | 17(56.67) | 15(50.00) | ||
Course of disease (year) | 6.70±1.09 | 6.33±0.92 | 1.408 | 0.164 |
BMI (kg/m2) | 21.88±1.59 | 21.91±1.40 | -0.095 | 0.925 |
GerdQ score | 13.70±1.54 | 13.27±1.48 | 1.112 | 0.271 |
SCL-90 scale | Control group (n=30) | Observer group (n=30) | Statistic | p | |
|---|---|---|---|---|---|
Somatization | Before nursing | 30.80±5.02 | 30.07±7.20 | t=0.458 | 0.649 |
Care for 3 months | 24.33±4.21 | 21.27±5.30 | t=2.484 | 0.016 | |
End of care | 22.40±3.74 | 19.83±3.28 | t=2.827 | 0.006 | |
Obsessive-compulsive symptoms | Before nursing | 34.47±6.91 | 33.50±7.08 | t=0.353 | 0.595 |
Care for 3 month | 28.20±5.53 | 26.53±5.63 | t=1.157 | 0.252 | |
End of care | 25.30±4.24 | 24.00±4.68 | t=1.128 | 0.264 | |
Interpersonal sensitivity | Before nursing | 27.53±6.22 | 27.10±6.41 | t=0.266 | 0.791 |
Care for 3 month | 26.40±4.67 | 24.00±4.63 | t=2.000 | 0.050 | |
End of care | 21.50±3.53 | 18.83±3.68 | t=2.865 | 0.006 | |
Depression | Before nursing | 40.23±7.31 | 40.63±7.32 | t=-0.212 | 0.833 |
Care for 3 month | 36.20±5.30 | 34.57±5.18 | t=1.207 | 0.232 | |
End of care | 30.40±6.26 | 26.43±4.70 | t=2.774 | 0.007 | |
Anxiety | Before nursing | 34.20±6.08 | 34.00±6.20 | t=0.126 | 0.900 |
Care for 3 month | 30.27±4.65 | 28.53±4.13 | t=1.527 | 0.132 | |
End of care | 29.03±4.12 | 23.47±4.32 | t=5.110 | <0.001 | |
Hostility | Before nursing | 20.27±4.14 | 19.80±4.04 | t=0.442 | 0.660 |
Care for 3 month | 17.27±3.50 | 15.47±3.19 | t=2.080 | 0.042 | |
End of care | 14.30±4.26 | 12.40±2.65 | t=2.075 | 0.042 | |
Terror | Before nursing | 24.33±4.63 | 24.50±4.50 | t=-0.141 | 0.880 |
Care for 3 month | 21.53±4.13 | 20.40±4.38 | t=1.031 | 0.307 | |
End of care | 17.53±5.32 | 14.57±4.13 | t=2.413 | 0.019 | |
Paranoia | Before nursing | 18.30±5.62 | 18.47±5.42 | t=-0.117 | 0.907 |
Care for 3 month | 15.30±3.67 | 13.83±3.52 | t=1.579 | 0.120 | |
End of care | 13.80±3.86 | 11.33±3.27 | t=2.668 | 0.010 | |
Psychosis | Before nursing | 26.97±3.50 | 27.20±3.42 | t=-0.261 | 0.795 |
Care for 3 month | 23.53±3.69 | 22.70±3.68 | t=0.876 | 0.385 | |
End of care | 20.10±3.25 | 16.23±3.66 | t=4.329 | <0.001 | |
Other | Before nursing | 22.53±4.67 | 22.57±4.55 | t=-0.028 | 0.978 |
Care for 3 month | 18.50±3.30 | 16.30±3.54 | t=2.489 | 0.016 | |
End of care | 15.57±3.18 | 12.93±2.66 | t=3.476 | 0.001 |
SF-36 scale | Control group (n=30) | Observer group (n=30) | Statistic | p | |
|---|---|---|---|---|---|
Physiological function | Before nursing | 53.50±12.01 | 54.03±11.36 | T=-0.177 | 0.860 |
Care for 3 month | 61.17±6.22 | 70.03±6.38 | T=-5.452 | <0.001 | |
End of care | 72.50±8.23 | 83.37±8.72 | T=-4.963 | <0.001 | |
Physiological role | Before nursing | 58.83±9.71 | 59.13±9.43 | T=-0.121 | 0.904 |
Care for 3 month | 68.27±6.80 | 76.37±7.15 | T=-4.497 | <0.001 | |
End of care | 72.60±8.20 | 84.20±7.85 | T=-5.596 | <0.001 | |
Physical pain | Before nursing | 54.53±9.10 | 53.27±9.33 | T=0.532 | 0.596 |
Care for 3 month | 65.47±9.60 | 71.20±10.13 | T=-2.251 | 0.028 | |
End of care | 73.93±10.33 | 84.00±8.45 | T=-4.133 | <0.001 | |
General health status | Before nursing | 55.13±10.89 | 55.83±10.37 | T=-0.255 | 0.800 |
Care for 3 month | 63.50±7.25 | 70.07±8.15 | T=-3.297 | 0.002 | |
End of care | 73.90±6.13 | 82.90±7.18 | T=-5.223 | <0.001 | |
Energy | Before nursing | 50.13±8.10 | 51.57±8.68 | T=-0.661 | 0.511 |
Care for 3 month | 64.57±7.30 | 72.73±7.54 | T=-4.263 | <0.001 | |
End of care | 75.40±6.77 | 82.63±6.37 | T=-4.262 | <0.001 | |
Social function | Before nursing | 54.77±8.64 | 53.50±8.44 | T=0.574 | 0.568 |
Care for 3 month | 61.97±6.89 | 73.30±6.38 | T=-6.613 | <0.001 | |
End of care | 74.70±6.35 | 80.70±6.42 | T=-3.639 | 0.001 | |
Emotional function | Before nursing | 52.20±9.30 | 50.90±9.56 | T=0.534 | 0.595 |
Care for 3 month | 64.23±8.72 | 74.77±7.26 | T=-5.084 | <0.001 | |
End of care | 71.87±5.16 | 81.07±6.46 | T=-6.096 | <0.001 | |
Mental health | Before nursing | 51.47±8.68 | 51.90±9.13 | T=-0.188 | 0.851 |
Care for 3 month | 63.17±6.15 | 73.47±7.18 | T=-5.965 | <0.001 | |
End of care | 73.97±7.89 | 83.80±6.22 | T=-5.364 | <0.001 |
PSQI scale | Control group (n=30) | Observer group (n=30) | Statistic | p | |
|---|---|---|---|---|---|
Sleep quality | Before nursing | 2.07±1.02 | 2.10±0.96 | t=-0.131 | 0.896 |
Care for 3 month | 1.60±1.07 | 1.63±1.03 | t=-0.123 | 0.903 | |
End of care | 1.37±1.10 | 1.43±0.97 | t=-0.249 | 0.804 | |
Time before falling asleep | Before nursing | 2.07±0.91 | 1.80±0.10 | t=1.084 | 0.283 |
Care for 3 month | 1.70±1.09 | 1.50±0.97 | t=0.750 | 0.456 | |
End of care | 1.63±1.10 | 1.37±1.07 | t=0.954 | 0.344 | |
Sleep time | Before nursing | 2.03±1.00 | 1.93±1.02 | t=0.385 | 0.702 |
Care for 3 month | 1.73±1.17 | 1.53±1.07 | t=0.689 | 0.494 | |
End of care | 1.77±1.14 | 0.90±0.85 | t=3.355 | 0.001 | |
Sleep efficiency | Before nursing | 2.00±1.05 | 2.47±0.82 | t=-1.919 | 0.060 |
Care for 3 month | 1.63±1.13 | 1.47±1.07 | t=0.568 | 0.560 | |
End of care | 1.30±1.18 | 1.17 ±1.18 | t=0.450 | 0.655 | |
Sleep disorders | Before nursing | 2.23±0.86 | 2.47±0.68 | t=-1.166 | 0.248 |
Care for 3 month | 2.07±0.87 | 1.70±0.99 | t=1.527 | 0.132 | |
End of care | 1.57±1.01 | 1.00±0.98 | t=2.207 | 0.031 | |
Hypnotic drugs | Before nursing | 1.70±1.09 | 2.10±1.03 | t=-1.463 | 0.149 |
Care for 3 month | 1.63±0.96 | 1.50±1.04 | t=0.514 | 0.609 | |
End of care | 1.50±0.97 | 0.97±0.89 | t=2.214 | 0.031 | |
Daytime dysfunction | Before nursing | 2.07±1.05 | 2.33±0.84 | t=-1.085 | 0.282 |
Care for 3 month | 2.00±0.95 | 1.50±1.23 | t=1.769 | 0.082 | |
End of care | 1.87±1.01 | 1.60±1.10 | t=0.978 | 0.332 |
Group | Eat too fast | Eat too much | Eating overheating | Spicy greasy | |
|---|---|---|---|---|---|
Control group (n=30) | Before nursing | 6 | 4 | 4 | 4 |
Observer group (n=30) | Before nursing | 5 | 3 | 6 | 2 |
<i></i>2 | 0.271 | ||||
p | 0.602 | ||||
Control group (n=30) | End of care | 5 | 2 | 3 | 4 |
Observer group (n=30) | End of care | 1 | 1 | 1 | 2 |
<i></i>2 | 6.239 | ||||
p | 0.012 | ||||
GERD | Gastroesophageal Reflux Disease |
MI | Motivational Interviewing |
PNI | Phased Nursing Interventions |
GerdQ | Gastro-oesophageal Reflux Disease Questionnaire |
CNI | Conventional Nursing Interventions |
IL-6 | Interleukin-6 |
TNF-α | Tumor Necrosis Factor-α |
IL-1β | Interleukin-1β |
CGRP | Calcitonin Gene-related Peptide |
5-HT | 5-hydroxytryptamine |
ELISA | Enzyme-linked Immunosorbent Assay |
RDQ | Reflux Disease Questionnaire |
SCL-90 | Symptom Checklist-90 |
GSES | General Self-Efficacy Scale |
SF-36 | Short Form-36 |
PSQI | Pittsburgh Sleep Quality Index |
BMI | Body Mass Index |
| [1] | Griffiths TL, Nassar M, Soubani AO. Pulmonary manifestations of gastroesophageal reflux disease. Expert review of respiratory medicine. 2020; 14: 767-75. |
| [2] | Zhang D, Liu S, Li Z, Wang R. Global, regional and national burden of gastroesophageal reflux disease, 1990-2019: update from the GBD 2019 study. Annals of medicine. 2022; 54: 1372-84. |
| [3] | Patel J, Wong N, Mehta K, Patel A. Gastroesophageal Reflux Disease. Primary care. 2023; 50: 339-50. |
| [4] | Maret-Ouda J, Markar SR, Lagergren J. Gastroesophageal Reflux Disease: A Review. Jama. 2020; 324: 2536-47. |
| [5] | Paul S, Abbas MS, Nassar ST, Tasha T, Desai A, Bajgain A, et al. Correlation of Anxiety and Depression to the Development of Gastroesophageal Disease in the Younger Population. Cureus. 2022; 14: e32712. |
| [6] | Bischof G, Bischof A, Rumpf HJ. Motivational Interviewing: An Evidence-Based Approach for Use in Medical Practice. Deutsches Arzteblatt international. 2021; 118: 109-15. |
| [7] | Beckwith VZ, Beckwith J. Motivational Interviewing: A Communication Tool to Promote Positive Behavior Change and Optimal Health Outcomes. NASN school nurse (Print). 2020; 35: 344-51. |
| [8] | Verma M, Horrow J, Navarro V. A Behavioral Health Program for Alcohol Use Disorder, Substance Abuse, and Depression in Chronic Liver Disease. Hepatology communications. 2019; 3: 646-55. |
| [9] | González-Lama Y, Ricart E, Cábez A, Fortes P, Gómez S, Casellas F. Medical consultation in ulcerative colitis: Key elements for improvement. World journal of gastroenterology. 2023; 29: 917-25. |
| [10] | de Freitas PP, de Menezes MC, Dos Santos LC, Pimenta AM, Ferreira AVM, Lopes ACS. The transtheoretical model is an effective weight management intervention: a randomized controlled trial. BMC public health. 2020; 20: 652. |
| [11] | Imeri H, Toth J, Arnold A, Barnard M. Use of the transtheoretical model in medication adherence: A systematic review. Research in social & administrative pharmacy: RSAP. 2022; 18: 2778-85. |
| [12] | Uzun S, Özmaya E. The effect of motivational interview conducted by nurses on quality of life: Meta-analysis. Perspectives in psychiatric care. 2022; 58: 2449-59. |
| [13] | Jones R, Junghard O, Dent J, Vakil N, Halling K, Wernersson B, et al. Development of the GerdQ, a tool for the diagnosis and management of gastro-oesophageal reflux disease in primary care. Alimentary pharmacology & therapeutics. 2009; 30: 1030-8. |
| [14] | Dent J, Vakil N, Jones R, Bytzer P, Schöning U, Halling K, et al. Accuracy of the diagnosis of GORD by questionnaire, physicians and a trial of proton pump inhibitor treatment: the Diamond Study. Gut. 2010; 59: 714-21. |
| [15] | Zhou J, Yu J, Zhou Y, Qiu J. Study of item text in the Chinese Symptom Checklist-90. Medicine. 2021; 100: e24841. |
| [16] | Brand E, Nyland J, Henzman C, McGinnis M. Arthritis self-efficacy scale scores in knee osteoarthritis: a systematic review and meta-analysis comparing arthritis self-management education with or without exercise. The Journal of orthopaedic and sports physical therapy. 2013; 43: 895-910. |
| [17] | Brazier JE, Harper R, Jones NM, O'Cathain A, Thomas KJ, Usherwood T, et al. Validating the SF-36 health survey questionnaire: new outcome measure for primary care. BMJ (Clinical research ed). 1992; 305: 160-4. |
| [18] | Zitser J, Allen IE, Falgàs N, Le MM, Neylan TC, Kramer JH, et al. Pittsburgh Sleep Quality Index (PSQI) responses are modulated by total sleep time and wake after sleep onset in healthy older adults. PloS one. 2022; 17: e0270095. |
| [19] | Li Q, Duan H, Wang Q, Dong P, Zhou X, Sun K, et al. Analyzing the correlation between gastroesophageal reflux disease and anxiety and depression based on ordered logistic regression. Scientific reports. 2024; 14: 6594. |
| [20] | Fuchs KH, Musial F, Eypasch E, Meining A. Gastrointestinal Quality of Life in Gastroesophageal Reflux Disease: A Systematic Review. Digestion. 2022; 103: 253-60. |
| [21] | Nasstasia Y, Baker AL, Halpin SA, Lewin TJ, Hides L, Kelly BJ, et al. Pilot Study of an Exercise Intervention for Depressive Symptoms and Associated Cognitive-Behavioral Factors in Young Adults With Major Depression. The Journal of nervous and mental disease. 2017; 205: 647-55. |
| [22] | Barsness KA, Bensard DD, Partrick DA, Calkins CM, Hendrickson RJ, Banerjee A, et al. IL-1beta induces an exaggerated pro- and anti-inflammatory response in peritoneal macrophages of children compared with adults. Pediatric surgery international. 2004; 20: 238-42. |
| [23] | Monu, Agnihotri P, Saquib M, Biswas S. Targeting TNF-α-induced expression of TTR and RAGE in rheumatoid arthritis: Apigenin's mediated therapeutic approach. Cytokine. 2024; 179: 156616. |
| [24] | Kilic F. Serotonin Signaling and the Hyperpermeable Endothelial Barrier in Sepsis: Clues to a Molecular Mechanism. Journal of community medicine & public health. 2024; 7. |
| [25] | Deshpande SN, Simkin DR. Complementary and Integrative Approaches to Prevention and Treatment of Child and Adolescent Obesity. Child and adolescent psychiatric clinics of North America. 2023; 32: 395-419. |
| [26] | Budhwani H, Naar S. Training Providers in Motivational Interviewing to Promote Behavior Change. Pediatric clinics of North America. 2022; 69: 779-94. |
| [27] | Chang CH, Chen TH, Chiang LL, Hsu CL, Yu HC, Mar GY, et al. Associations between Lifestyle Habits, Perceived Symptoms and Gastroesophageal Reflux Disease in Patients Seeking Health Check-Ups. International journal of environmental research and public health. 2021; 18. |
| [28] | Beauvais C. Motivational interviewing to improve treatment adherence. Joint bone spine. 2019; 86: 535-7. |
| [29] | Cole SA, Sannidhi D, Jadotte YT, Rozanski A. Using motivational interviewing and brief action planning for adopting and maintaining positive health behaviors. Progress in cardiovascular diseases. 2023; 77: 86-94. |
| [30] | Chen H, Wang Y, Liu C, Lu H, Liu N, Yu F, et al. Benefits of a transtheoretical model-based program on exercise adherence in older adults with knee osteoarthritis: A cluster randomized controlled trial. Journal of advanced nursing. 2020; 76: 1765-79. |
| [31] | Selçuk-Tosun A, Zincir H. The effect of a transtheoretical model-based motivational interview on self-efficacy, metabolic control, and health behaviour in adults with type 2 diabetes mellitus: A randomized controlled trial. International journal of nursing practice. 2019; 25: e12742. |
| [32] | Li X, Yang S, Wang Y, Yang B, Zhang J. Effects of a transtheoretical model - based intervention and motivational interviewing on the management of depression in hospitalized patients with coronary heart disease: a randomized controlled trial. BMC public health. 2020; 20: 420. |
| [33] | da Rosa MC, Rosa CB, Boff RM, Oliveira MS, Schwanke CHA. Transtheoretical model for lifestyle changes in older persons: a systematic review protocol. Annals of the New York Academy of Sciences. 2022; 1508: 172-7. |
APA Style
Zhuo, L., Zhang, D., Xiang, W., Liu, T., Ding, Y. (2026). A Prospective Analysis of the Effects of Motivational Interviewing Combined with Phased Nursing Interventions on Patients with Gastroesophageal Reflux Disease. Clinical Medicine Research, 15(1), 6-18. https://doi.org/10.11648/j.cmr.20261501.12
ACS Style
Zhuo, L.; Zhang, D.; Xiang, W.; Liu, T.; Ding, Y. A Prospective Analysis of the Effects of Motivational Interviewing Combined with Phased Nursing Interventions on Patients with Gastroesophageal Reflux Disease. Clin. Med. Res. 2026, 15(1), 6-18. doi: 10.11648/j.cmr.20261501.12
@article{10.11648/j.cmr.20261501.12,
author = {Li-Li Zhuo and Daguan Zhang and Wei-Xiao Xiang and Tian-Na Liu and Yin-Rong Ding},
title = {A Prospective Analysis of the Effects of Motivational Interviewing Combined with Phased Nursing Interventions on Patients with Gastroesophageal Reflux Disease},
journal = {Clinical Medicine Research},
volume = {15},
number = {1},
pages = {6-18},
doi = {10.11648/j.cmr.20261501.12},
url = {https://doi.org/10.11648/j.cmr.20261501.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cmr.20261501.12},
abstract = {Objectives: To evaluate the effects of MI combined with PNI on the quality of life, self-efficacy, psychological state, and sleep quality of patients with GERD. Methods: 60 GERD patients were enrolled based on inclusion and exclusion criteria and randomly assigned to the observation (30 cases) or control groups (30 cases). The observation group underwent MI combined with PNI, while control group received conventional nursing interventions. The changes in inflammatory response-related indicators were compared between two groups. The reflux disease questionnaire (RDQ), symptom self-rating scale (SCL-90), self-efficacy scale (GSES), simple SF-36 scale and Pittsburgh sleep quality index scale (PSQI) were employed to assess the patient's conditions before, three months following and after nursing. Results: Baseline inflammatory markers and scale scores showed no significant between-group differences. After 3 months, the observation group demonstrated significant reductions in these inflammatory markers compared with baseline and the control group. At the same time point, SCL-90 scores decreased across multiple domains, GSES scores improved, and SF-36 scores increased in several dimensions. PSQI scores were also significantly lower in the observation group, indicating better sleep quality. Conclusion: MI combined with PNI may reduce inflammation, relieve negative emotions, and enhance self-efficacy, quality of life, and sleep in GERD patients.},
year = {2026}
}
TY - JOUR T1 - A Prospective Analysis of the Effects of Motivational Interviewing Combined with Phased Nursing Interventions on Patients with Gastroesophageal Reflux Disease AU - Li-Li Zhuo AU - Daguan Zhang AU - Wei-Xiao Xiang AU - Tian-Na Liu AU - Yin-Rong Ding Y1 - 2026/04/23 PY - 2026 N1 - https://doi.org/10.11648/j.cmr.20261501.12 DO - 10.11648/j.cmr.20261501.12 T2 - Clinical Medicine Research JF - Clinical Medicine Research JO - Clinical Medicine Research SP - 6 EP - 18 PB - Science Publishing Group SN - 2326-9057 UR - https://doi.org/10.11648/j.cmr.20261501.12 AB - Objectives: To evaluate the effects of MI combined with PNI on the quality of life, self-efficacy, psychological state, and sleep quality of patients with GERD. Methods: 60 GERD patients were enrolled based on inclusion and exclusion criteria and randomly assigned to the observation (30 cases) or control groups (30 cases). The observation group underwent MI combined with PNI, while control group received conventional nursing interventions. The changes in inflammatory response-related indicators were compared between two groups. The reflux disease questionnaire (RDQ), symptom self-rating scale (SCL-90), self-efficacy scale (GSES), simple SF-36 scale and Pittsburgh sleep quality index scale (PSQI) were employed to assess the patient's conditions before, three months following and after nursing. Results: Baseline inflammatory markers and scale scores showed no significant between-group differences. After 3 months, the observation group demonstrated significant reductions in these inflammatory markers compared with baseline and the control group. At the same time point, SCL-90 scores decreased across multiple domains, GSES scores improved, and SF-36 scores increased in several dimensions. PSQI scores were also significantly lower in the observation group, indicating better sleep quality. Conclusion: MI combined with PNI may reduce inflammation, relieve negative emotions, and enhance self-efficacy, quality of life, and sleep in GERD patients. VL - 15 IS - 1 ER -
Department of Gastroenterology, First Affiliated Hospital of Wenzhou Medical University, Wenzhou, China
Figure 1. Flow chart of the study.
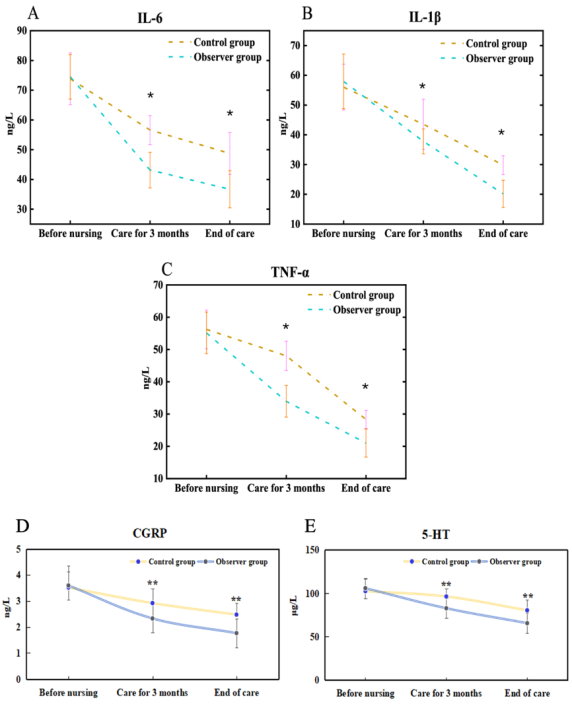
Figure 2. Comparison of Changes in Inflammatory Response.
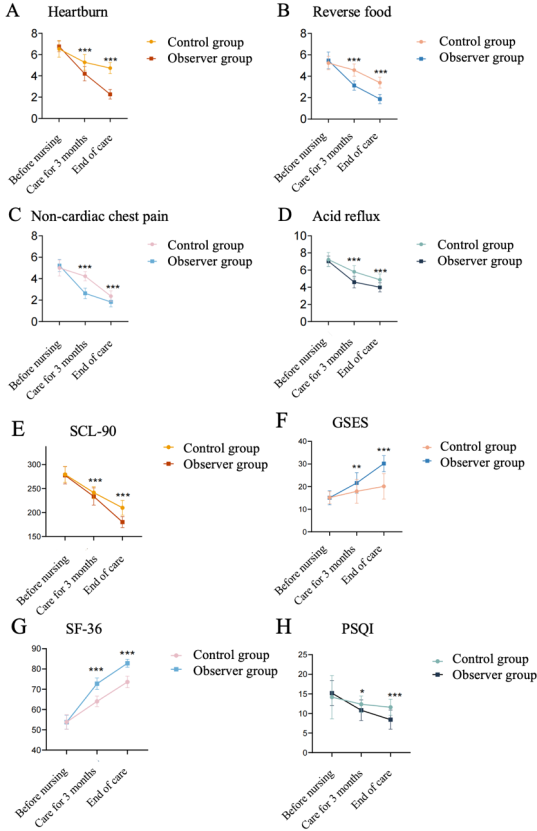
Figure 3. Comparison of different clinical observation indicators A-D Comparison of RDQ scores for heartburn (A), dysphagia (B), non-cardiac chest pain (C), and acid reflux (D) between the control and observation groups; E-H Comparison of RDQ scores for SCL-90 (E), GSES (F), SF-36 (G), and PSQI (H) between the control and observation groups (*p < 0.05; **p < 0.01; ***p < 0.001).
Information

